

Test to see if a GLP-1 drug is right for you
Test to see if a GLP-1 drug is right for you
Volume 9, Issue 5 | February 1, 2024


In This Issue
Yes, we can eradicate TB - here’s how
. . . and we can do it for cervical cancer, too
Why bother retesting PCR-positive COVID patients?
Hair gives a heads-up for potential birth complications
New and Noteworthy
TB eradication in sight if cheaper tests more widely available
Tuberculosis (TB) has been an endemic human scourge since humans first inhabited towns and villages. While it is now treatable, the challenge is making sure that it gets diagnosed, as its progression is often asymptomatic … until it is too late.
While TB has largely been eliminated in developed countries (except for multidrug-resistant pockets), it causes 11 million cases and 1.3 million deaths per year in the developing world. According to a feature in Nature this week, it could be eradicated there, as well, if the novel diagnostics described in the piece can be brought to bear. These range from blood tests that utilize nanoparticles engineered to bind to one of the proteins the microbe produces to urine tests that look for the same proteins to good old-fashioned radiography (only digital and AI-assisted), and more. All that is missing, the author argues, is money and political will.
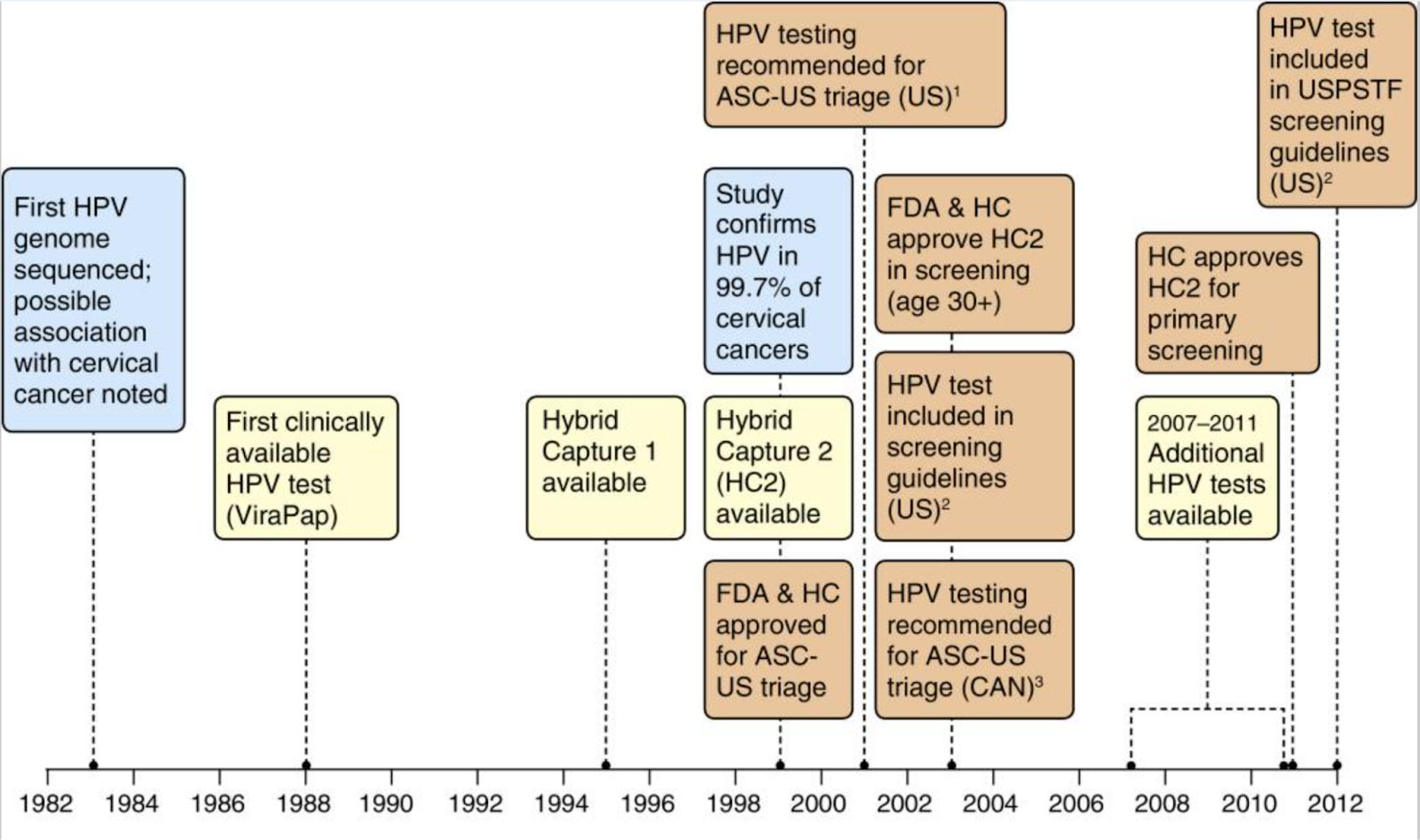
Dx + HPV vaccines will = extinction of cervical cancer
As was widely reported last week, Public Health Scotland reported that after 35 years of health tracking, not a single woman who was vaccinated against human papillomavirus (HPV) at age 12 or 13 ended up developing invasive cancer. Not one.
This is a happy ending to a story that began with diagnosis. It started with the Pap smear in 1949, then continued in 1976, when Harald zur Hausen (2008 Nobel) theorized that a virus was the primary cause of cervical cancer. The genomic revolution later allowed cost-effective molecular tests for that virus, and in 2006 the first vaccine was licensed. Today, diagnostic innovation focuses on mRNA tests, since these indicate the extent of cellular infection.
Commentary: We now know that the combination of HPV vaccination and diagnostics is fully capable of eliminating 99% of cases, but here in the US only half of teenagers are currently vaccinated. We must get all pre-teens of both sexes fully covered.
Most rtPCR-positive COVID patients don’t need to be retested
Once someone tests positive for SARS-CoV-2 (the virus that causes COVID) on rtPCR, is it worth testing them again to see if they’re still contagious? For years, the conventional wisdom has been that it’s not, and a recent retrospective study in Scientific Reports bears that out - with a couple of caveats.
The take-homes:
Seven days after an initial positive result, 90.5% of patients still tested positive (i.e., with a Ct value < 30). Ct value (Cycle threshold) is a quantitative measure of viral load. As explained by the CDC: The lower the Ct value (meaning, the fewer cycles needed to turn a test positive), the greater the amount of viral RNA present in the original sample. In contrast, high Cts nearer to the assay’s limit of detection (often ~40 cycles) indicate trace amounts of viral RNA in the tested sample.
When a first test was only borderline positive, Ct values often rose in subsequent tests, indicating a decreased viral load. This most likely occurred because these patients were already on the path to recovery at first testing.
Commentary: rtPCR is an almost perfect test for the presence of viral RNA (both intact virus and non-viable fragments). But without Ct values, that test has two major flaws: It can’t catch patients in the early asymptomatic days because results take too long to arrive, and it remains positive long after the infectious period has ended. Nevertheless, this data does support two important conclusions:
It’s a good idea to report Ct values along with the binary positive/negative result, because a borderline result might indicate convalescence.
If you test positive you are probably still infectious for longer than the five days suggested by regulatory bodies.
Food for Thought
Should you hop on the anti-obesity-drug bandwagon? A test may tell you
The GLP-1 anti-obesity drugs Ozempic, Wegovy (both semaglutide), Zepbound, and Mounjaro (both tirzepatide) are blazing hot right now. So much so that demand has been outstripping supply in some cases. But like all drugs, they come with side effects, and oh by the way they ain’t cheap. So wouldn’t it be nice to know if there was another drug that - for you - would work even better, for less money and with fewer side effects?
One biotech company is betting you can find out. According to research published in Obesity by the company’s founders in 2021, what you need to know is whether you have a “hungry gut” - a stomach that quickly empties and wants to be filled again. If that’s your problem, then GLP-1 drugs are probably the right choice. If you have other issues - a “hungry brain” that doesn’t realize you’ve eaten enough, a low resting metabolic rate, or you’re an emotional eater - other, cheaper medications are more likely to help. And you’re not only likely to lose more weight if your doc prescribes medication according to one of these four “obesity phenotypes” (1.7x more weight loss after a year; 79% of phenotype-guided patients lost >10% of body weight in a year, versus 34% of patients whose treatment wasn’t guided by phenotype). According to the (small) study, if you’re prescribed a GLP-1 drug based on your phenotype, you’re also less likely to experience unpleasant side effects (14% in phenotyped group; 34% in non-phenotyped group).
With their scientist hats on, the study authors acknowledge that bigger studies with a more diverse pool of subjects are needed to bolster these results. But when they put on their entrepreneurial caps, they aren’t waiting for confirmation. The company is marketing a genomic test (AI-based, because 2024) that ostensibly tells you which phenotype you have.
Commentary: Assuming that the research holds up, adding this test to the process makes perfect sense from a medical perspective. But fads are hard to fight. It may be a while before people stop coming into doctors’ offices asking for the latest thing in weight loss.
Hair samples may predict birth complications
Predicting challenges and complications around pregnancy and childbirth is tough to do. Pregnancies that are known to be high-risk are tracked carefully, but average-risk pregnancies - not so much.
Researchers have found a way to get a heads-up when what looks like an average-risk pregnancy may actually be one on which to keep a closer eye. In a small study of 53 pregnant people, they measured cortisol in hair samples. In some of those folks, the levels of that hormone were elevated - an indication of increased stress over the previous three months. Of that group, 25% (13) later experienced unpredicted birth complications, such as early birth or maternal hemorrhaging.
Of note: In addition to taking hair samples, the researchers asked women to complete a survey about their perceived stress level. The survey results did not correlate with birth complications - only the cortisol level in hair did.