



Mid-summer update: Blood tests for Alzheimer’s and colon cancer
Volume 10, Issue 4 | August 1, 2024


In This Issue
Wastewater - where are we now?
Steady improvements in AI for pathology
Bird flu update
New and Noteworthy
FDA approves first blood-based screening test for colon cancer
This week the FDA approved Shield, the first blood-based colorectal cancer screening test, for people over 45 with average risk. The test’s clinical trial (20,000-plus subjects) showed ~83% sensitivity and 90% specificity (the major stool-based test, Cologuard, has a sensitivity of ~92%). However, Shield doesn’t score in that range for early disease. As its required label notes, it “has limited detection (55 percent to 65 percent) of Stage I colorectal cancer and does not detect 87 percent of precancerous lesions. One out of 10 patients with a negative Shield result may have a precancer that would have been detected by a screening colonoscopy."
Commentary: While Shield’s accuracy is not as high as either colonoscopy or Cologuard, we believe that a blood test will capture people who should get tested but refuse to have a colonoscopy or use a stool-based test.
Alzheimer’s diagnosis: Is this the blood test we’ve been looking for?
We’ve written a lot this year about tests that aim to diagnose Alzheimer’s disease by measuring p-tau217 levels in blood. The trick, it seems, has been to figure out exactly which p-tau values one should look for, and what other markers should be combined with those to make an accurate test. This week, a JAMA study has received a lot of press for presenting a blood test that (air quotes) diagnoses Alzheimer’s with 90% accuracy. Yup, you read that right. Here are some details.
The test combines two measurements in plasma: The ratio of phosphorylated tau 217 (p-tau 217) to non-phosphorylated tau 217 and the ratio of amyloid-β 42 to amyloid β-40. pTau217 alone was very effective but when the two were combined, they increased overall diagnostic accuracy to 88 - 92%. Dementia specialists, by comparison, had an overall diagnostic accuracy of 72%, with primary care docs only a few points behind.
Commentary: The paper was presented at the Alzheimer’s Association International Conference, where it came with a flotilla of caveats: The test should only be used in people with cognitive impairment, because there’s no treatment yet for folks in earlier stages; it should be performed after tests like CT have ruled out other causes such as stroke; it should be confirmed with follow-up tests. All valid points, and yet 90+%! Of course caveats are appropriate given the scope of this study, but the real value of these blood tests is in identifying the earliest cases for clinical trial and eventual therapy development. We’re finally getting somewhere.
Where we are on wastewater
Before the pandemic, most people had never heard of wastewater surveillance - for infectious disease or anything else. By the time the public health emergency ended in 2023, some of us had learned to rely on it for early detection of COVID trends. Last week, COVID journalist Betsy Ladyzhets published an overview of the current state of COVID wastewater surveillance in the US in The Sick Times, a website dedicated to cover Long COVID issues and promote activism.
The key takeaways:
Wastewater, although imperfect, is the only broad measure we have today to estimate current incidence COVID across the US.
Many institutions that were focused on wastewater analysis are either testing fewer sewer systems or reporting on them less frequently, due to lack of resources.
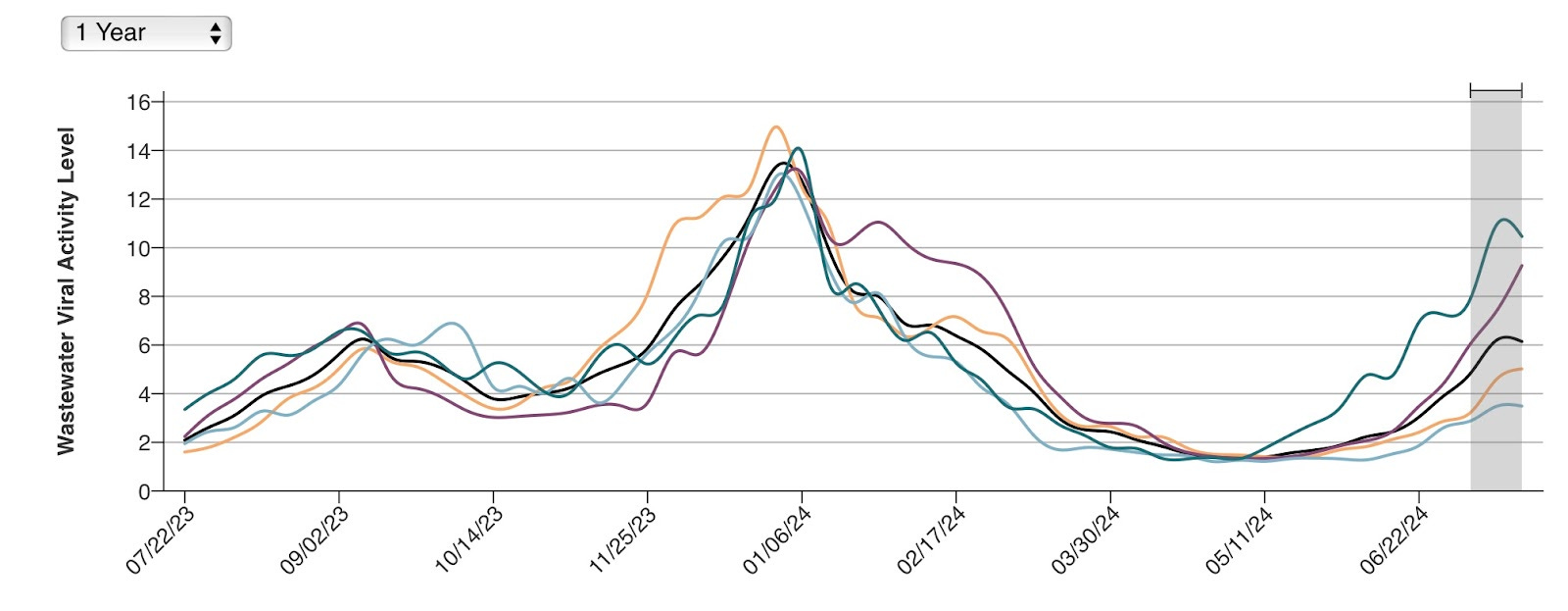
The CDC’s wastewater dashboard is the most comprehensive today. See below for a chart of viral activity levels over the past year. (Hard to miss the current summer surge.)

Bird flu update: CDC test flaw; flu shots for farm workers
Three more Colorado poultry workers have tested positive for H5N1. Fourteen human cases of the virus have now been documented in the US, all with mild symptoms. According to HealthBeat, about 45 people in the country have been tested for the virus thus far.
The only currently authorized test for H5N1 is the one from the CDC - and it has a problem. As originally designed, the test does work. However, as KFF News described it, “a flaw emerged when a company contracted by the agency manufactured the tests in bulk. In these tests, one of two components that recognize proteins called H5 in the H5N1 bird flu virus was unreliable.” Because the other component still works well, the CDC went ahead and distributed the tests to labs - with instructions to consider the test inconclusive unless both components register a positive result.
The CDC plans to buy $5 million worth of seasonal flu shots to be offered to farm workers at risk of H5N1 infection. They will spend an additional $5 million promoting vaccination in that population. While those shots will not protect people from bird flu, they should decrease the chance that a worker gets infected with both H5N1 and the seasonal human strain at the same time.
Food for Thought
Deep disease insight improves AI for pathology
A recent Ground Truths blog from Eric Topol features an interview with Faisal Mahmood, discussing how Mahmood’s Mass General/Brigham team is developing a more accurate and practical AI system to carry out tissue analysis. Over the past six months this group has published several articles on AI pathology, culminating in a Nature paper (online this week). Among many insights discussed:
“Weakly supervised” AI is superior to “strongly supervised” learning – it skips laboriously annotating every possible feature in an image, leaving AI deep learning to join the dots between an image and a diagnosis.
Pathology-specialized AI is 50% better than general or medically focused AI (PathChat was correct 79% of the time, versus runner-up GPT4V at 52%)
Analyzing 3D blocks of tissue (not just 2D slices on a glass slide) enables better diagnosis but generates so much data that only AI has the time to review it. (5/2024 Cell paper)
Adding non-destructive imaging (e.g., microCT) enables more tissue from a biopsy to be examined, with less damaging pre-processing. It eliminates the error-prone process of deciding which tiny part of the tissue is put on a slide for viewing, and allows subsequent tests to be performed without a repeat biopsy.
Adding clinical (text) data to the learning set improves accuracy by 8-10% beyond using the image alone.
Making the AI easy to access enables faster pathologist adoption – as does calling PathChat an AI “copilot or companion.”


Commentary: These advances are compelling, especially when this becomes a clinically practical package (PathChat is not quite there yet). As the chart here shows, the current pathology paradigm involves considerable inaccuracy: Three of six pathologists were correct only 2/3 of the time, and even when an entire organ’s worth of tissue was available, diagnoses were incorrect about 20% of the time.
Developing effective AI for pathology is harder than it is for radiology and cardiology. In those specialties, data is captured digitally from the beginning, whereas currently, pathology slides have to be imaged as an additional step. Another big remaining challenge is the sheer quantity of memory and processing power required to implement these AI systems. The 3D approach described uses a lot of clever compression and selection techniques but still requires two to three orders of magnitude more data and processing than other techniques do. Still, progress is very exciting – better diagnoses delivered faster, and in more locations.
Quick Hits
Last week we talked about screening the Seine river for disease-causing microbes in preparation for the Olympics. Good thing it’s being done - over the weekend, despite the $1.5 billion Paris spent on cleaning up the long-polluted river, tests revealed levels of E. coli too high for safe swimming. So what happened? Downpours during Friday’s opening ceremony washed sewer waste into the waterways - a chronic problem in big cities with limited runoff areas. Fortunately, the tests showed clean water on Wednesday, allowing the triathlon to take place. Triomphe!
COVID & COVID/Respiratory EUA Update
The FDA issued no new COVID 510(k) premarket notifications, one new EUA, six amendments to existing EUAs, one new revocation and no warning letters in July.
510(k) Premarket Notifications: 0
COVID / Respiratory Panels: 0
New EUAs: 1
COVID / Respiratory Panels: 1 (Nano-Check Influenza+COVID-19 Dual Test)
Amendments to Existing EUAs: 6
Molecular: 4
Antigen: 2
Revocations/ Warning Letters: 1
Is Shield cheaper than Cologuard? What is Cologuard's send/spec numbers for Stage 1/2?