



Feature Focus: Liquid Biopsy
Volume 9, Issue 8 | February 22, 2024


Liquid biopsy goes back to basics
The first approved liquid-biopsy test was fairly simple: It counted cancer cells in the blood to track tumor burden and recurrence (CellSearch in 2012). These days, the vast majority of liquid biopsies don’t bother isolating scarce circulating tumor cells (CTCs). Instead, they use increasingly inexpensive next-generation sequencing to differentiate tumor from non-tumor cell-free DNA (cfDNA) present in the bloodstream.

However, a small number of recently published approaches buck the trend. The big advantage of going back to a CTC-first approach is that intact cells can be investigated more completely. For example, you can measure cancer-cell population diversity more precisely and can look at biomarkers that are only available within an intact cell. Two cases in point: A brain-cancer test that looks for circulating glial cells (covered below in this Newsletter) and a test that helps determine whether lung nodules seen on imaging are cancerous by looking for “circulating genetically abnormal cells.”
Commentary: Whether it makes sense to go CTC-first depends on the specific cell / tissue / organ dynamics of each tumor type and the clinical value of the additional data gained. The amount of clinically valuable data available from cfDNA keeps on growing, so it is likely that CTC-first approaches will only make sense where cfDNA fails to provide necessary accuracy (e.g. where RNA transcription and protein translation enhance clinical relevance). However, it’s worth remembering that thus far both the CTC and cfDNA approaches have not yet demonstrated value in early (pre-symptomatic) screening due to their lower yield in earlier stage, pre-metastatic cancer. We will see…
A blood test for glioblastoma? Really?
Brain cancers span a range of different types, each with their own treatments (gliomas, glioblastomas, astrocytomas, oligodendrocyte cancers), so knowing which is which matters. Imaging is the initial means to diagnose symptomatic/functional neurological issues. However, a high-risk biopsy is the only definitive diagnostic technique that can determine whether mass in the brain is benign or not. While 70 to 80% of brain tumors are not malignant, up to 40% of these masses cannot be biopsied (nor can they be surgically removed).
Two recent papers describe blood tests that, for certain types of brain cancer, could remove the need for a traditional biopsy. One describes a circulating glial cell (CGC) diagnostic with a claim of almost perfect analytical accuracy for diagnosing glioblastoma in spiked and patient 20ml blood draws: 99.35% sensitivity and 100% specificity. The other looks at the palette of proteins in blood taken from vessels near a glioma and compares that to the proteins in blood from other locations in the body.
Commentary: It is extraordinary that glial tumor cells even migrate across the blood-brain barrier in sufficient quantity to be detected in the body (limit of detection here is roughly one cancer cell per ml), although recent work reports newly discovered ways cells can do that. Cancers that begin in the brain typically do not find a further location in which to metastasize, so it may be that these particular cells are doomed to circulate for the rest of their (un)natural lives. Exciting, almost too good to be true - we look forward to additional studies.
Using liquid biopsy to monitor cancer treatment success
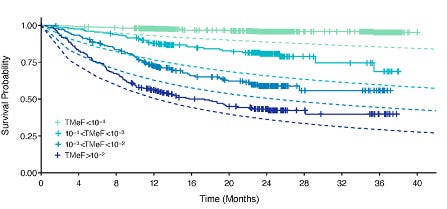
Declaring a cancer patient’s treatment a success is challenging because cancer cells that could potentially drive recurrence are currently impossible to detect below a certain threshold (MRD – Minimal Residual Disease). For blood/lymphatic cancers the situation is more straightforward, though not foolproof: Any sample is highly likely to detect the presence of new cancer cells. For solid tumors, repeat biopsy can only be used after PET/CT imaging detects newly formed tumors - which can’t be found until they are bigger than a relatively large ~4mm (1/6 of an inch). A recent paper (Figure 6b reproduced here) describes using increased methylation in circulating tumor DNA (tumor methylation fraction above 1 in 10,000, aka TMeF>10-4) to monitor recurrence. Additionally, TMeF patterns differ by tissue/molecular type, providing important clues to evolving resistance.
Commentary: Liquid biopsy has limitations, too. An oversimplification: The shedding of circulating tumor DNA into the bloodstream is dependent on tumor size, location, and degree of vascularization. We will be covering more research in this area in the coming months.
UK study controversy highlights MCEDs’ weakness: Low PPV
Screening an otherwise healthy population for cancer using a Multiple Cancer Early Diagnostic (MCED, the British version of the US’s MCD mentioned above) can generate far more false than true positives, giving such a test low positive predictive value (PPV). On the other hand, it can be very useful as a test to rule out cancer in patients with ambivalent symptoms, as long as the negative predictive value is high enough (although that often comes at the cost of more false positives – it’s a challenging balancing act).
With that background, the UK’s National Health Service (NHS) has begun a large clinical pilot using one particular MCD beginning this year. A Lancet letter raised an objection, claiming that spending up to $19 billion on this program was inappropriate given current screening performance, and suggesting bias in test selection.
The chair of the NHS’ Cancer Mission program responded in the same Lancet issue. He stated that finding ways to diagnose cancer at earlier stages is essential, especially given growing incidence in the 50-77 year age group, and that the pilot will cost a small fraction of a full roll-out while providing real-world data for future efforts.
Commentary: We estimate the pilot will cost about $420 million: 140,000 patients, tested each year for three years, at ~$1,000 per test. The outcome will be carefully evaluated by US payors and will no doubt impact US insurance policies.
Are pan-cancer tests worth it? New NIH network to find out
On the other side of the pond, NIH’s National Cancer Institute has launched a nationwide, multicenter program to evaluate multi-cancer detection assays (MCDs) in general. The Cancer Screening Research Network, coordinated by the Fred Hutchinson Cancer Center in Seattle, will start this year with a pilot study of up to 24,000 subjects. The goal: To figure out if it’s possible to do an even bigger randomized controlled trial that settles the questions of whether the benefits of MCDs outweigh the costs, and whether they actually reduce deaths or not.