Extended imaging aims to decrease stroke recurrence
Volume 12, Issue 9 | August 7, 2025


ALSO IN THIS ISSUE
Diagnosing the root cause of dementia with AI
UK doctors skeptical of self-tests
AI trained on one culture might not work in another
Bird Flu: Infectious virus is airborne and in farm wastewater
Measles: Texas outbreak slowing, more outbreaks arise

AI tool aims to diagnose the root cause of dementia
The neurodegeneration that drives progressive dementia and disability comes in many different forms. In order to begin treatment and give the patient their prognosis, busy clinicians need to be able to reliably pinpoint the root cause of neurodegeneration in that particular patient. This week, STAT News covered StateViewer, a cloud-resident image-analyzing AI tool from the Mayo Clinic that aims to provide exactly that information. A more detailed exploration appeared in Neurology (paywall) earlier this year.
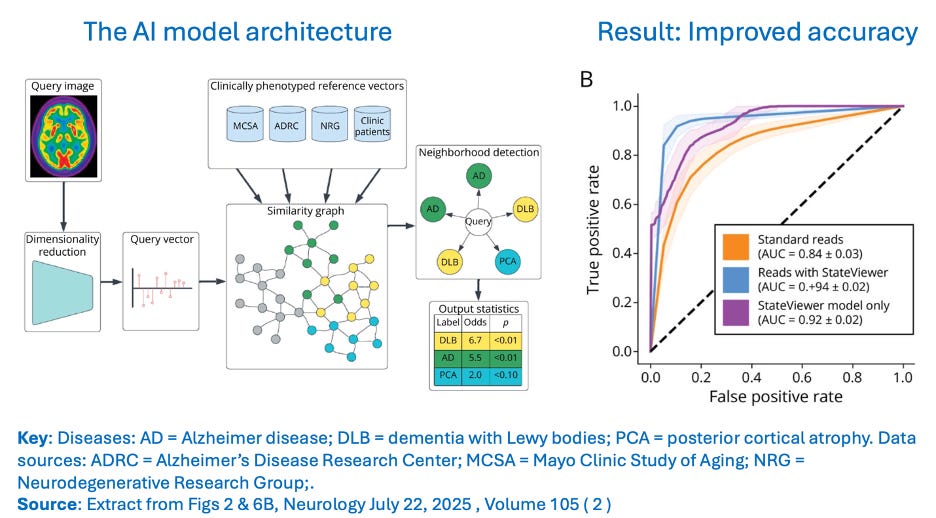
COMMENTARY: The tool provides considerably enhanced accuracy even in a clinical environment as advanced as Mayo’s. In less-sophisticated systems, it is likely to deliver even more substantial diagnostic improvements. But as always, there are caveats.
As STAT News points out, many academic and commercial initiatives are bringing the power of AI to the diagnosis of neurodegenerative disease. The strength and weakness of this tool is that it uses only FDG-PET brain scans as input. (FDG-PET uses short-lived radioactive tracer injections to highlight where glucose is being consumed in the brain - those locations are where the brain is using energy.) That’s a strength because energy use in the brain is the most direct evidence of normal versus defective brain function. But it’s also a weakness, because PET-FDG is an expensive imaging tool not widely available outside major hospitals. The tool also ignores (at least for now) valuable insight that could be gained from other data in patients’ medical records as well as input from other more easily accessed diagnostic tools, from written tests to plasma protein concentrations.
Major reductions in stroke recurrence from minor change in imaging
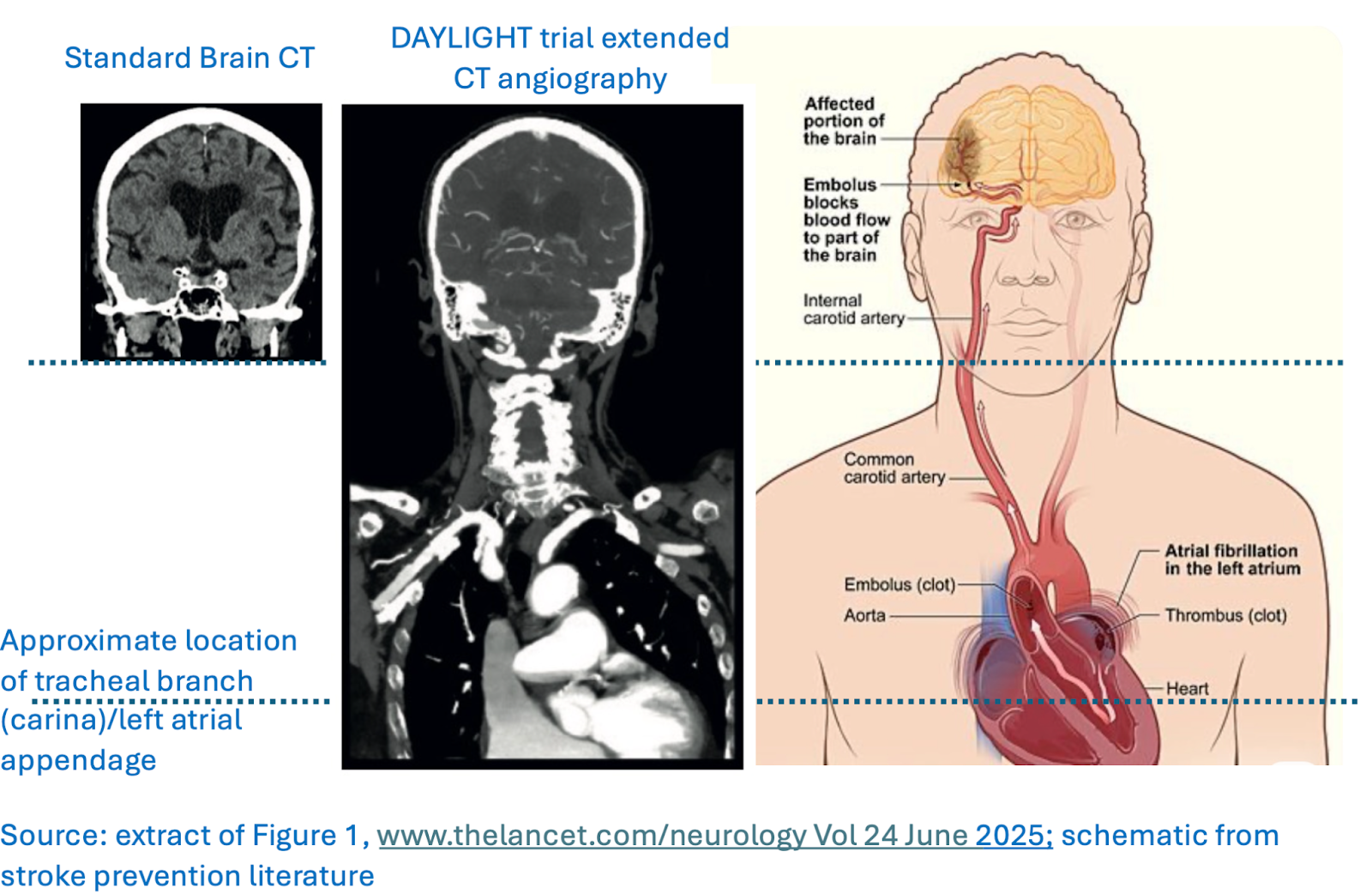
Increasing the area imaged in suspected strokes could improve diagnosis of one specific cause of stroke by nearly 6x while only increasing the imaging time from 20 to 21 minutes, according to recent research in The Lancet Neurology. The imaging tool in question is computerized tomographic angiography (a CT scan that uses contrast material so that you can see the blood vessels).
Scientists compared the results they got when stroke patients received standard head-and-neck CT angiography to what they found when scans continued lower into the chest to the level of the heart’s atria (see image). The result? The extended scans found additional clots waiting in the heart or aorta in 20 of the 226 patients who got extended scans, versus just 4 in the 239 receiving standard scans.
COMMENTARY: Stroke is a major cause of disability in those over age 65. But it is often underestimated, underdiagnosed, and consequently undertreated at its earliest stages when treatment can make a difference.
Most strokes (87%) are caused by clots that block blood vessels, cutting off the blood supply to a part of the brain. The heart is the source of about 30% of these clots, so it makes sense to look at the heart and its vessels to see if another clot is lurking there, waiting to cause the next stroke.
Early treatment with blood thinners is highly effective for treating strokes, but patients and physicians both tend to ignore the early warning signs until they recur, often catastrophically. Bottom line? Don’t ignore signs of stroke – limb weakness, difficulty speaking/understanding, decreased vision, and lack of coordination, especially if only on one side of the body – even if they seem to go away. Get treatment promptly, and if you have had a stroke or suspect you are having one, insist on getting extended CT angiography to help prevent the next one.

UK doctors skeptical of self-tests – in some cases, for good reason
The BMJ (the UK’s equivalent to the NEJM) just published a set of articles that are broadly critical of having so many over-the-counter tests available in UK supermarkets. The package included two research reports together with a feature, How safe are health tests on UK supermarket shelves? and an editorial, The pitfalls of diagnostic self-tests.
One of the research reports evaluated 30 tests for 19 different health conditions. It found that 60% were “inaccurate and/or unsuitable for public use,” citing, for example, test instructions that included using a centrifuge and storing samples in -20°C freezers (not equipment frequently found in British kitchens or any kitchen). The editorial draws a distinction between yes/no tests that are easy to understand (e.g., pregnancy and HIV tests) and those with complex or subtle instructions and / or dubious clinical utility. The feature picks out a rogues’ gallery of four self-tests and their challenges:
A follicle-stimulating hormone test to diagnose menopause (the implications of a result vary across the menstrual cycle)
A test that looks for small amounts of a protein called albumin in the urine, to evaluate kidney function (the result is useless without looking at the ratio of albumin to another protein, creatinine)
Vitamin D (the results are too hard to read)
A thyroid-stimulating hormone test to evaluate thyroid function (the test instructions are in the wrong order, and the user could have a health issue even if their levels are fine)
COMMENTARY: Regulatory oversight of self tests in Europe has traditionally been less stringent than it is in the US, for better or worse. Since the 1980s, CE marking has been required to sell diagnostics in the EU (and the UK, which was in the EU for 50-plus years). This marking certifies that a diagnostic test is in compliance with all EU regulations, but since manufacturers self-certify, new products can be launched very quickly (in a matter of weeks).
Some of the tests these articles highlight do indeed have fundamental issues, especially when a single result taken out of context doesn’t give the user enough information to draw conclusions. Others are useful and appropriate, they’re just poorly executed.
All that said, self-testing and self-collection is growing because consumers want more convenient and lower-cost access to important health information. The answer is not to stand against progress - remember, it was not so long ago that many doctors argued that women could not be trusted to use pregnancy tests. Instead, we should make the right accurate tests available, and get them right.
If you train your AI on one culture, it might not work in another
Earlier this summer, NEJM AI reported an AI screening tool for Parkinson’s disease that can diagnose the condition with impressive – though not exceptional – 89% accuracy (77% sensitivity and 91% specificity). It works by detecting the flat facial affect in response to emotions that is typical of the disease, called hypomimia. The algorithm was trained on patients and controls in the US, and an odd thing happened when researchers tested it on people in Bangladesh at high risk of the disease. The tool’s positive predictive value (the likelihood that someone who tests positive actually has the disease), which was 73% in the US, declined to 36%.
COMMENTARY: AI is especially vulnerable to bias, partly because it cannot know more than what it was trained upon, and partly because how it draws conclusions is hidden from view. That means AI developers must curate their training sets very carefully. Both depth and relevance of training data are of paramount importance.

Bird Flu: Research indicates infectious virus is airborne
Research published in a preprint this week demonstrated that infectious virus is airborne on dairy farms with infected cows. Scientists tested the breath of individual cows as well as the air within milking parlors and barns, and also used an air-sampling device that simulated the exposure that dairy workers receive. The same preprint also noted that wastewater on these farms, some of which is reclaimed and used to clean milking equipment and dairy parlors, also contained active virus. Previous research had indicated that milk and contact with contaminated milking equipment was the primary way the virus was transmitted among cattle and to people. These discoveries indicate that the virus may spread in other ways, as well.
Measles: Texas outbreak slowing, but more outbreaks arise
No new cases of measles have been reported in Texas for the past two weeks. However, the virus was detected in wastewater on July 21 in the city of Austin, suggesting that infections there have not been reported.
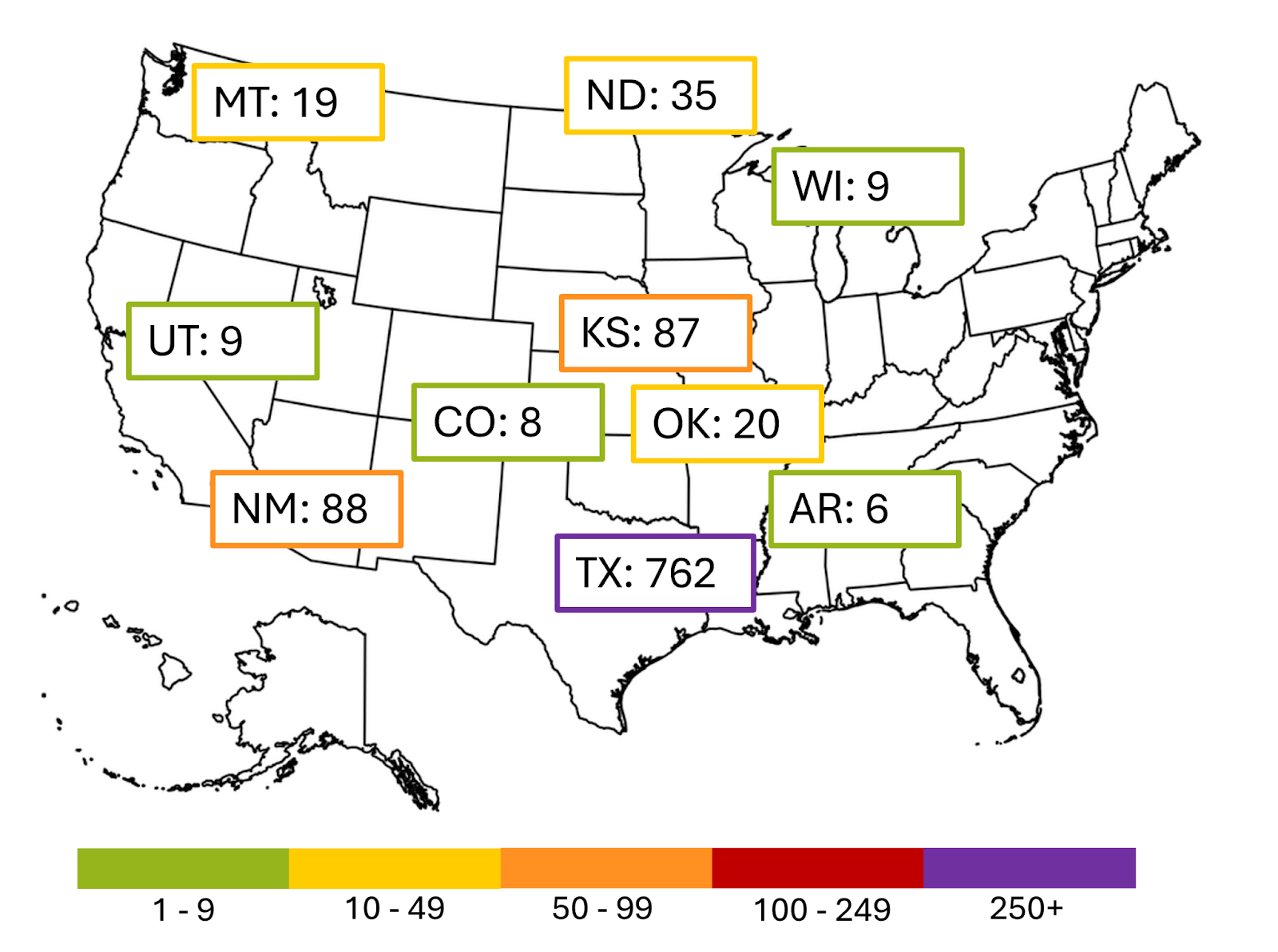
As of now, 1,356 confirmed cases of measles have been reported in the US this year - the highest number in over 30 years. There have been 32 outbreaks in the nation so far in 2025 - 2024 saw only 16 during the entire year. Canada, which has roughly one-eighth the population of the US, is in even worse shape, with 4,206 probable and confirmed cases. Mexico’s outbreak falls between the two, at 2,597. The vast majority of all cases have happened in unvaccinated people (86% of the cases in Canada, 92% in the US).
The current larger outbreaks are shown below. The cases in Texas, New Mexico, Kansas, and Oklahoma all came from the same source; those in Arkansas, Colorado, Montana, North Dakota, Utah, and Wisconsin are unrelated.