



COVID vs. Flu - Round 3
Volume 7, Issue 6 | February 8, 2023


IN THIS ISSUE
India’s diagnostics “catapult”
Wastewater as asymptomatic screening tool
What the end of the PHE means for test reporting and reimbursement
Is “individual responsibility” effective against COVID?
Keeping an eye on avian flu
New and Noteworthy
India launches diagnostics “catapult” to prepare for next pandemic
As COVID is moving into an endemic phase (otherwise known as the “We are stuck with this forever” phase), conversation is shifting to future pandemics. Earlier this month, India’s Centre for Cellular and Molecular Platforms (C-CAMP) of India announced a diagnostics-focused initiative both to increase pandemic preparedness and to establish “a global model for capacity-building in the diagnostics domain in lower- and middle-income countries.”
The initiative, funded by The Rockefeller Foundation, Gates Foundation, and FIND, builds on C-CAMP’s 2020 COVID success: In one year, they were able to increase testing capacity in India to one million PCR tests per day throughout the country. That work was made possible through the establishment or expansion of more than 200 Centers of Excellence and the development of 40+ approved PCR tests and 12 rapid antigen tests. Commentary: We hope that this initiative will be a model for other countries, which should all be thinking beyond COVID. The time to establish or solidify networks that will be able to identify and then test for future pathogens is now. Note: Mara is an advisor to The Rockefeller Foundation.
Food for Thought
Wastewater testing can be both sensitive and specific
Okay, we admit it: We’re kind of obsessed with wastewater. And as is the case with so many nerdy pursuits, we’re part of a small but passionate tribe. If you, too, think wastewater testing could be the Next Big Thing in virus surveillance, we have two great articles for you, both by Betsy Ladyzhets of the COVID-19 Data Dispatch.
Her piece in The Atlantic focuses on airplane wastewater testing, which we’ve discussed here before. But that’s just the tip of the pile. In an article on her website, she reviews the possibilities for wastewater testing at K-12 schools, congregate living facilities, health care facilities, large communal workplaces (think meat-packing plants and manufacturing lines), and neighborhoods. Commentary: Wastewater surveillance in these places offers the possibility of physically non-invasive, sensitive asymptomatic testing. And the beauty is that it’s not scattershot - it’s focused specifically on communities at high risk of infectious-disease outbreaks. If you’re looking to get a lot of bang for your testing buck, hold your nose and collect some poop.
The end of the PHE: Test reporting, reimbursement, and telehealth
Since last week’s announcement about the end of the Public Health Emergency, there have been many questions about what will happen - and commentary about what should happen.
To oversimplify, the questions have been revolved around three areas:
Data reporting to the federal government. What will states be required to submit to HHS? As a result of that, what will be available for surveillance and early detection of outbreaks of COVID and new pathogens? The COVID-19 Data Dispatch did an excellent job in detailing the options and potential outcomes.
What will happen to the cost / reimbursement coverage of tests, vaccines, and treatments? Medscape had a simple list of the most likely scenarios. Bottom line - No more 100% free options from the federal government, with a few exceptions (oral antivirals for Medicare recipients, and testing and treatments for Medicaid).
What will happen to telehealth? For Medicare, it will continue through December 2024.
How well does “individual responsibility” work against COVID?
For nearly a year, the official line on COVID prevention has been one of “individual responsibility.” A recent model-based preprint seeks to answer a vital question about that tactic: How well does it work? And if not everyone is bothering to try to avoid getting COVID, what does an individual who does want to avoid infection have to do?
The answer, not surprisingly, is pretty sobering. If you’re vaccinated, you do have less of a chance of getting infected than if you’re not. However, if you want to decrease your infection frequency by 50% (from 1.3x yearly to 0.65x), you’ll need to have 10x fewer contacts than the median. If you don’t take any measures to avoid infection, be prepared to spend about a week a year sick with COVID - and to run a 12% risk of contracting Long COVID, as well.
Commentary: This model - which assumes, among other things, that COVID is endemic - also suggests that somewhere between 32 and 66 million adults in the US will have long COVID at any given moment in time. June 2022 Census data indicates that of folks who currently have the syndrome, about 12.5% are out of work due to the condition. If you add those lost work hours to the aggregate loss due to acute COVID, that’s an awful lot of lost economic activity, not to mention the personal cost. I guess we’re willing to pay that price, huh? Seems kinda steep.
Looking for a way around qPCR’s biggest flaw
The great strength of qPCR is also its weakness: Its exquisite sensitivity identifies not only functional virus, but also post-infectious viral fragments that can’t possibly replicate. A recent preprint suggests a way around the problem: Adapt PCR primers to detect only the complementary strand to the positive RNA viral genome. Since it’s only present during viral replication, this “anti-genome” should only be picked up when an active infection is present. Commentary: The approach discussed is suggestive, but it’s neither definitive nor comprehensive, and other PCR targets that might achieve this same objective (e.g., sub-genomic RNAs) are not evaluated in this paper. Nevertheless, finding novel ways to benefit from PCR’s sensitivity without its Achilles heel is a noble and achievable objective.
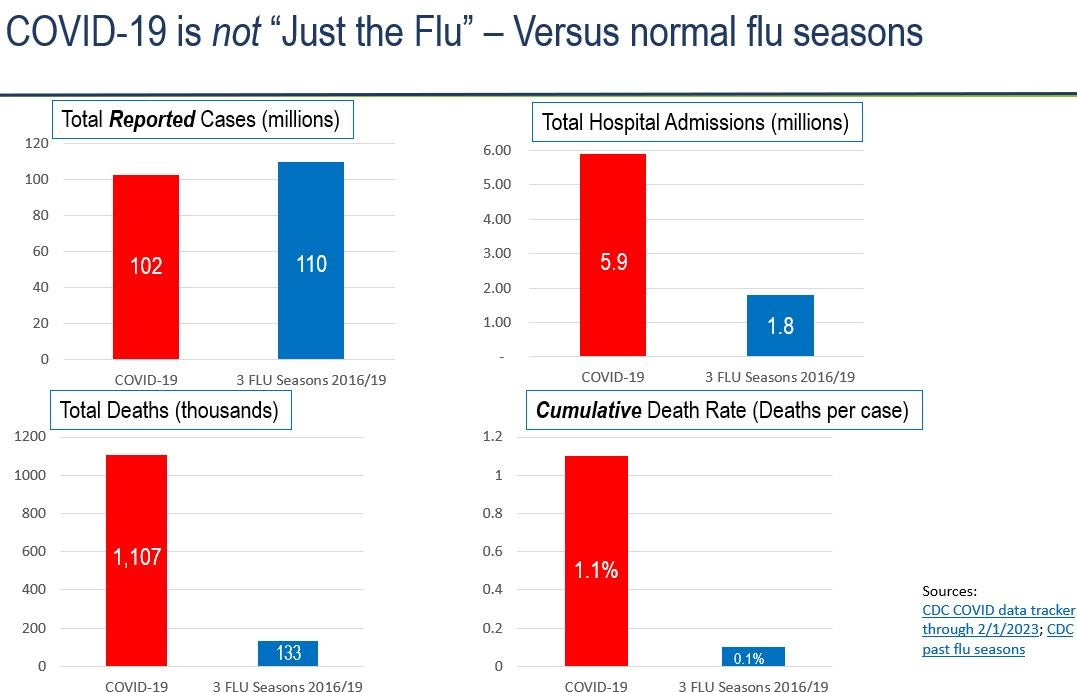
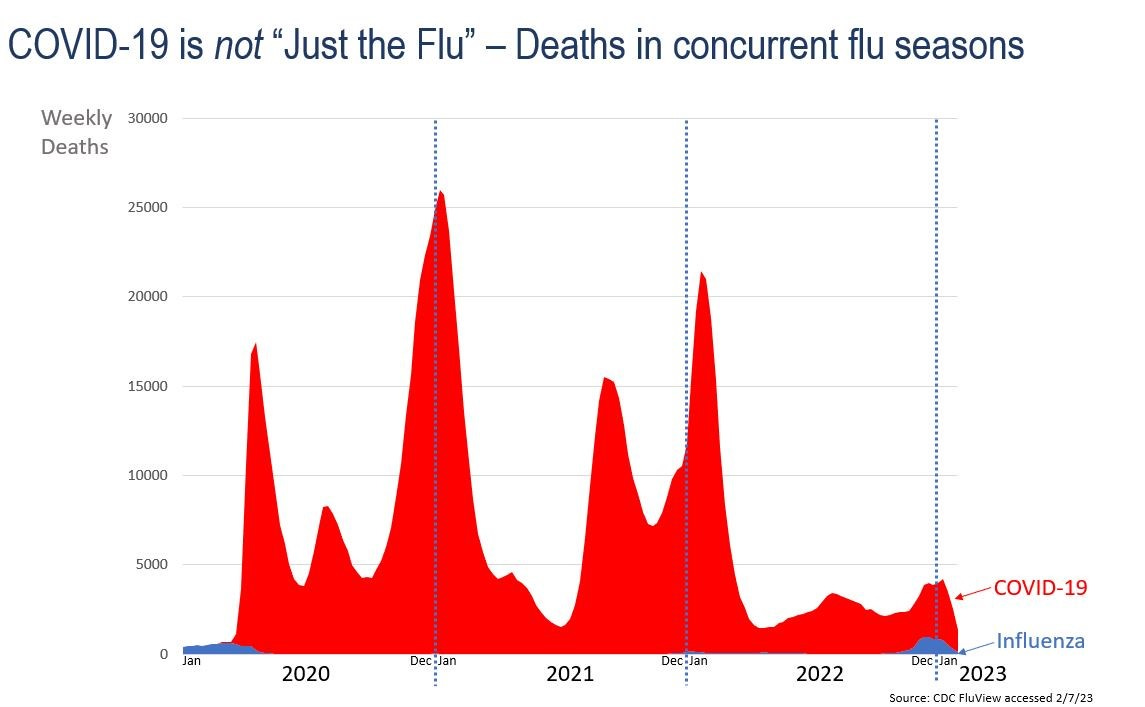
Lest we forget… COVID deaths are ~10x higher than “normal” influenza
COVID has now been with us for three full years, and over that time has killed over 1.1 million people in the US - a case fatality rate (CFR) of 1 - 2% (the reported CFR number is 1.1%, but undercounting of cases persists). To put this CFR in context, influenza has a “normal” CFR of 0.1% (that’s the three-season pre-COVID average from 2016-19).
COVID precautions quashed the 2020 - 21 and 2021 - 22 flu seasons, which was a welcome reprieve. But as you can see in the charts below, those precautions and their benefits disappeared this winter.
Bird (flu) watching
Speaking of influenza, we’ve noted a flock of recent articles on avian flu (H5N1) this week. More on this topic in the future, but here are a few insights that appear to be shared amongst many scientists to date:
H5N1 is unpredictable. It has showed its face in the past but then stuck its head back in the sand for years.
It has infected a wide number of animals over time, including mammals - mink, foxes, seals, and others.
Testing and aggressive action is critical now to eradicate spread within infected animal communities.
Testing needs to include humans who have had any contact with infected animals.
Commentary: We are trying not to worry too much about avian flu, despite the alarmingly high CFR (70 to 90%). But we have to say that even our two prior coronavirus epidemics could have been much worse had they spread more widely, and their CFRs weren’t nearly as bad (2003 SARS: 10%, 2012 MERS: 34%). We cannot take avian flu lightly.
Quick Hits
According to a report in JAMA Neurology, a simple blood test (P-tau217) was highly predictive of cognitive decline due to preclinical Alzheimer’s disease over six years of follow-up. This test promises to be a far superior diagnostic as compared to past tests ( which have advanced from autopsy to amyloid PET imaging to CSF collection) and may drive long-awaited development of effective therapies.