



Biden’s Dx highlights challenges with prostate-cancer screening
Volume 11, Issue 21 | May 22, 2025


ALSO IN THIS ISSUE
Improving MS diagnosis and prediction of progression
A (small) step toward a test for bad eating habits
Data behind HPV self-collection device released
Get the CRC Dx stats right, please
Bird flu and measles updates: Mostly good news

A (small) step toward a test for bad eating habits
According to current estimates, over 40% of US adults are obese, and on average, 50% of our bodies’ energy needs are supplied by ultra-processed foods (UPF). Those statements aren’t just related - there’s evidence that our UPF intake is causing our obesity problem.
Yet without a reliable diagnostic test for levels of UPF consumption, it is hard to provide individual health guidance. (Yes, you can ask people what they’re eating, but a) we often won’t remember, and b) we are often . . . less than completely truthful.)
Research in PLOS Medicine offers a potential solution. Scientists used mass spectrometry to analyze blood and urine samples from over 700 adults ages 50 - 74 who recorded what they ate. They were able to identify a set of metabolites that represented UPF consumption. (Don’t worry, this whole thing was validated later with younger folks who were randomized into groups that ate prescribed diets.) As the Associated Press reported, “From those, they devised a score of 28 blood markers and up to 33 urine markers that reliably predicted ultra-processed food intake in people consuming typical diets.”
COMMENTARY: More work required. Metabolomic panels like this have two challenges. One is the enormous complexity of the metabolites we create, the other is that mass spectrometry is a time-consuming and expensive technique (although as interest in metabolomics rises, new and simpler approaches are becoming available). In addition, the research doesn’t offer any diagnostic-ready evaluation of effectiveness (sensitivity, specificity, etc.) This is an important field, but unfortunately, this paper only lays some groundwork for a test.
Data behind first FDA-approved HPV self-collection device released
Last week we reported on the first FDA-approved device that allows women to collect their own samples for human papilloma virus (HPV) testing. This week, the company that makes the device released the results of the clinical trial behind the approval. The study ultimately included 582 women, and test sensitivity for self-collected and clinician-collected samples was equivalent, at about 96%.
When talking about cancer Dx, get the stats right, please
Cases of colorectal cancer (CRC) have been rising dramatically over the past couple of decades. Last week, National Geographic published an excellent summary of a Nature paper that might explain why that’s happening (childhood exposure to a toxin produced by certain gut microbes), but the statistics in that Nat Geo article scared the bejeezus out of us.
As originally published, the article stated that “one in five people under age 54 is diagnosed with the disease.” Yikes! That would be about 40 million cases a year - a truly terrifying number.
A few days later, Nat Geo corrected the statistic. It’s not that one in five people under 54 get diagnosed with CRC - it’s that one in five cases of CRC happen in people under age 54. See the difference? It matters, because that number is a thousand times smaller, at about 35K per year, or about 0.017% of people under age 54. Whew!

Bird Flu Update: Why no recent human cases?
Why have human bird flu cases disappeared in the US? As the Associated Press reported, “The most recent infections confirmed by the CDC were in early February in Nevada, Ohio, and Wyoming.” Nobody knows the answer to this question, but experts note that:
Now that the spring bird migration is over, bird flu cases in animals have decreased.
Immigrant farm workers with mild symptoms are likely to avoid getting tested for fear of being deported.
It’s unlikely that severe cases are happening without being reported.
While some surveillance for the disease does continue, the amount of work being done in this area has decreased significantly due to cuts and resignations at USDA and FDA.
Measles: Texas outbreak slowing
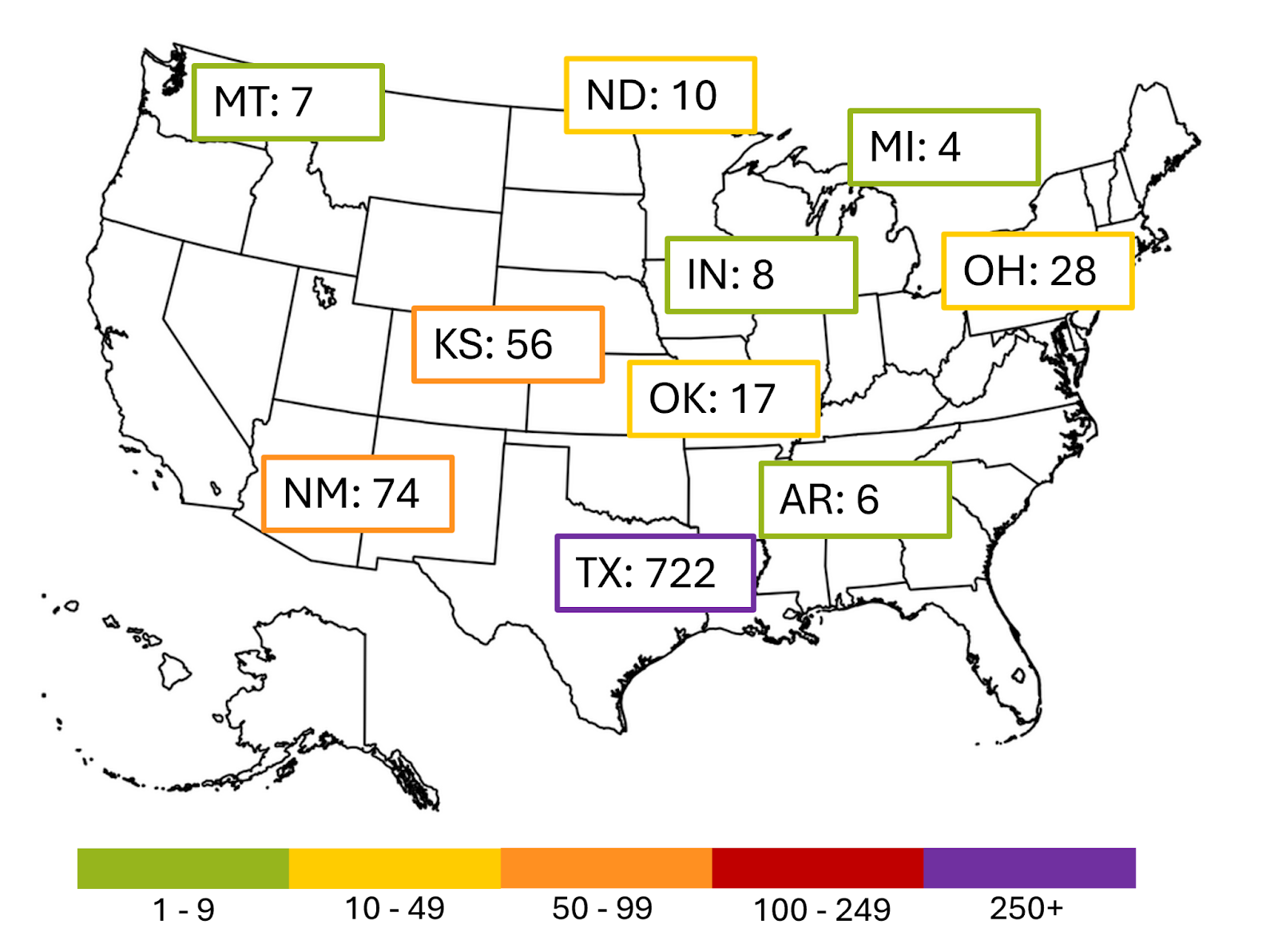
While the outbreak in Texas has not ended, it does appear to be slowing down. As CIDRAP reports, “Based on rash-onset dates,” cases have been declining since a peak in mid-March.”
The current larger outbreaks are shown below. The cases in Texas, New Mexico, Kansas, and Oklahoma all came from the same source; those in Arkansas, Indiana, Michigan, Montana, North Dakota and Ohio are unrelated.

COMMENTARY: Biden’s Dx highlights need for prostate-cancer screening
President Biden’s late-stage cancer diagnosis has gotten a lot of people talking about prostate-cancer screening. Since the 2010s, cases of advanced prostate cancer in the US have risen somewhere between 4% and 6.5% per year (the number depends on what set of years you’re talking about and which data set you’re using). Experts say that’s probably happening because of decreased screening.
COMMENTARY: So why did the amount of screening go down? Because screening guidelines and recommendations didn’t keep up with changes in how prostate cancer is diagnosed and managed.
A recent STAT News article (paywall) does a lovely job of laying out the details, but the tl;dr version is this: A well-publicized 2009 trial found that screening with the prostate-specific antigen (PSA) test did not decrease the number of deaths due to prostate cancer. Because of this, the US Preventive Services Task Force downgraded its recommendation for the test, saying that both its monetary and physical costs (resulting in unnecessary biopsies, etc.) generally outweighed its benefits.
At that point, many doctors stopped recommending the PSA test, even though:
The trial turned out to have significant problems.
MRI emerged as a useful follow-up to the PSA test, reducing the biopsy burden for many men
Clinicians started to use “watchful waiting” instead of aggressive treatment for early-stage cancers - especially for men over 70, as prostate cancer in older men is typically slow-growing
It’s also important to note that according to the American Cancer Society, most men diagnosed with prostate cancer do not die from it. Indeed, studies have shown that 70% of men over 70 years old have cancerous cells in their prostate glands - but it doesn’t kill the vast majority of them.
Our take: The PSA test is notoriously inaccurate, with a high false positive rate, but if a man is generally healthy and can psychologically handle watchful waiting without undue stress, then he should ask his doctor for the test.
Improving MS diagnosis and progression prediction
Diagnosing multiple sclerosis (MS) is often a challenging and invasive process. There is no single definitive test; instead, diagnosis typically goes from clinical evaluation to MRI of the brain and from there to lumbar puncture / spinal tap, an invasive and painful procedure. (Researchers in the UK argue that they can get a clear diagnosis without that spinal tap from a specialized, T2-weighted MRI.)
Even after a patient has been diagnosed, it is also challenging to predict when they will progress from relapsing / remitting MS (stable except for episodes of deterioration) to the progressive stage, when symptoms get steadily worse. Typically the call is made about three years after the transition between stages actually began. That’s important because most current MS meds only work during the relapsing stage.
Researchers in Sweden have developed an algorithm that analyzes a patient's existing medical history - past blood tests and imaging data - to predict when that transition might occur. In the study, based on medical records from 22,000 MS patients, the algorithm diagnosed progression correctly or early in 87% of cases.
The algorithm has a particularly helpful feature: It tells the clinician how confident it is in its diagnosis - so the physician can decide whether the score is worth using or not. An anonymized version of the model is available online.
How reliable is CGM in non-diabetics?
Continuous glucose monitors (CGM) have revolutionized care for insulin-dependent diabetics. By monitoring glucose levels in real time, they can warn users about either rising or falling glucose levels before potential health crises occur. However, these days, it seems like all the cool non-diabetic kids are using wearables to manage general health, diet, and exercise, and that includes CGMs. (Yeah, we know - we didn’t expect our field to become hip, either.)
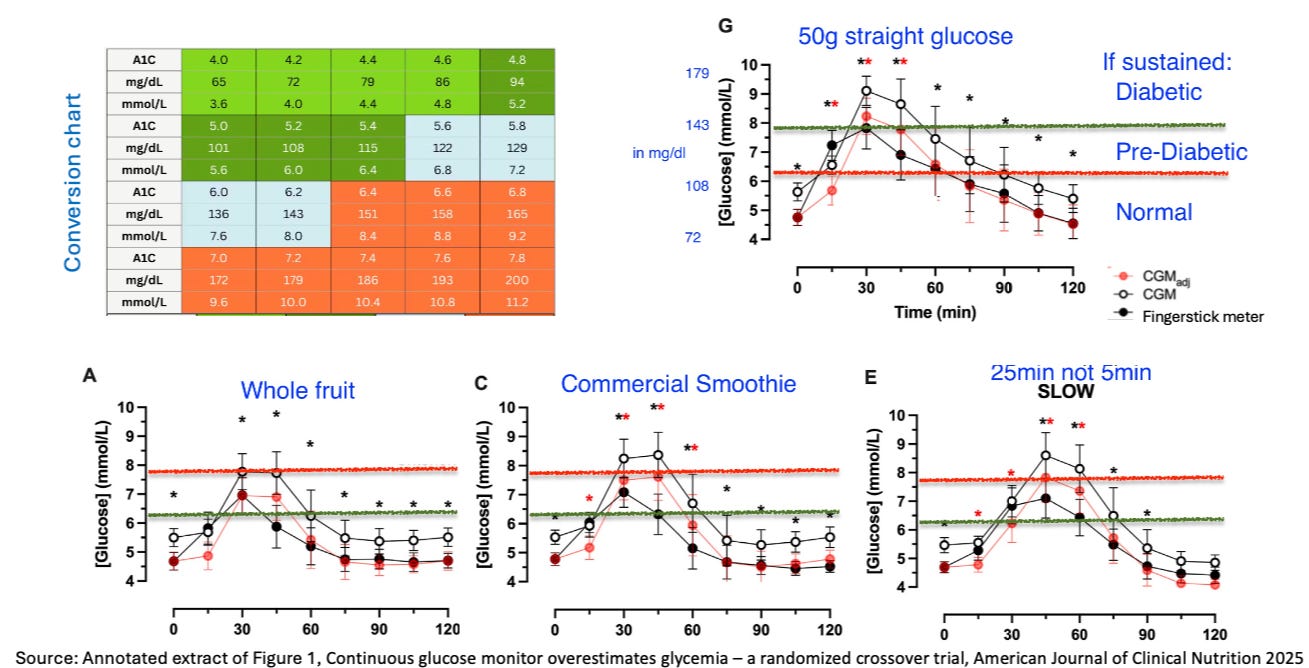
But these devices weren’t developed for non-diabetics. Can we assume that they work just as well for these people? Data published in the American Journal of Clinical Nutrition implies that they don’t. Instead, it shows that these devices systematically overestimate glucose levels and their duration, implicitly suggesting that wearers take corrective measures which may be unnecessary and might be harmful.
Before we dig in, some caveats. This trial is very small (n=15), was conducted in a highly controlled environment, and covers the devices of only one manufacturer.
Nevertheless (see annotated figure below), CGM-reported glucose levels were on average 22mg/dl higher than the more accurate fingerstick (with an upper limit of normal at about 136mg/dl, this is a significant issue). About 10mg/dl of this difference came from simple miscalibration by the manufacturer (presumably fixable). About 12mg/dl of the difference happened because the devices reported spikes that were higher and longer-lasting than those reported by fingerstick. (In healthy individuals, spike height and duration are by far the biggest contributors to high average glucose levels.)
COMMENTARY: Researchers and clinicians are increasingly focused on spotting pre-clinical signals of chronic and slow-to-develop disorders, so non-diabetic glucose patterns are getting increasing attention. For the pre-diabetic, CGMs offer key information that can prompt improved management of diet and exercise and the introduction of first-line drug therapy (GLP1, metformin, etc.). However, if the work of this paper holds up to further scrutiny, it raises a serious question about how CGMs should be used for people not at risk of impending diabetes.
Systematically overestimating glucose levels in the healthy, particularly immediately after eating, may lead to unnecessary, even unachievable glucose-management goals. For non-diabetic folks, HbA1c is a better option. It monitors average glucose levels over the past few months, avoiding the unnecessary anxiety caused by (inaccurate) minute-to-minute monitoring.

Nature recently updated its Outlook on Medical Diagnostics. Its two newest articles are an argument for performing whole-genome sequencing in diagnosing rare diseases and a summary of the challenges and opportunities of multi-cancer early detection tests.
We hope that you enjoy the long issue this week. We will be off next week for Memorial Day.