



To get AI to recognize rare diseases, teach it what’s common
Volume 10, Issue 20 | November 21, 2024


IN THIS ISSUE
Making diagnosis sweeter - with lollipops
Bird flu: Concerning mutations; POC test coming
Will POC test get heart-attack patients to treatment more quickly?
The challenge of diagnosing early-onset cancer
Happy almost Thanksgiving! We’ll be taking off next week to roast, bake, eat, and repeat.
We wish you and yours a joyous and savory holiday.

Lollipop Dx: Because we all need news that’s fun
Nobody likes a throat swab. And if you think that’s uncomfortable, consider what it’s like to get a mouth biopsy. Now imagine that instead of having to go through either of those, you could get a diagnosis by sucking on a lollipop.
It’ll be a while before doctors’ offices are stocked with diagnostic candies, but the idea is more than a Wonka-inspired dream. Lollipops that collect saliva samples for strep throat have been successfully tested in humans. Ones that use smart hydrogels to collect proteins for cancer diagnosis are a ways behind, just going through the proof-of-concept stage.
Now, who’s working on Wonka’s fizzy lifting drinks?
Bird flu: Concerning mutations in Canadian case; POC test in development
The strain of bird flu that infected a teenager in British Columbia has mutations that “would make it easier for that version of H5N1 to infect people,” STAT News reports. Scientists think the mutations arose in the patient during their infection, and the strain does not appear to have been transmitted to anyone else. The teen remains in critical condition.
The CDC has signed an agreement to develop a rapid molecular test for flu A, flu B, and H5 flu in humans. While current tests must be processed at a central lab, the new test is intended for use “at the point of need - beyond just the clinic setting,” CIDRAP reported.
Yesterday, Pennsylvania began requiring bulk milk testing for avian flu. It is only the fourth state that has not experienced an H5N1 outbreak in cattle to require such testing. The others are Arkansas, Massachusetts, and Oklahoma.

Will a new POC test reduce time to treatment for heart attacks?
When a patient arrives at the ER with chest pain, one of the possible causes that must be investigated ASAP is a heart attack. In a classic heart attack, also called a type 1 myocardial infarction (type 1 MCI), a vessel within the heart muscle is blocked. The longer that blockage persists, the more muscle dies. On the other hand, there are many possible causes of chest pain that are either not urgent or not heart-related at all.
As part of ruling out type 1 MCI, physicians use the high-sensitivity cardiac troponin test (PATHFAST hs-cTnI-II). Until recently, that involved sending blood to a hospital lab, so test turnaround time could be anything from 20 to 40 minutes. This fall, the FDA approved the first point-of-care (POC) device that can run the test, so it could be done right there in the ER itself.
COMMENTARY: Placing another sophisticated device in an ER has downsides. You have to find a place to put the thing, have a staff member available to run it, and spend time on quality control, maintenance, and staff training. Several FDA-approved central (stat) lab tests for hs-cTn already exist, and at least three POC tests are already used in Europe (see this 2022 review). Will this new test truly shorten time to treatment?
For it to do so, physicians must believe that a single hs-cTn test is adequate to rule out MCI. Hs-cTn is very sensitive for MCI, but not unique to it (low specificity), so high levels may result from other non-urgent or chronic conditions (e.g., kidney failure). Changing the location of this one test may not make that much of a difference.
To get AI to recognize rare diseases, teach it what’s common
One of the great benefits of AI is that it remembers everything that it has ever seen, and never fails to notice when it sees those things again. But how do you get AI to flag something it’s never seen before?
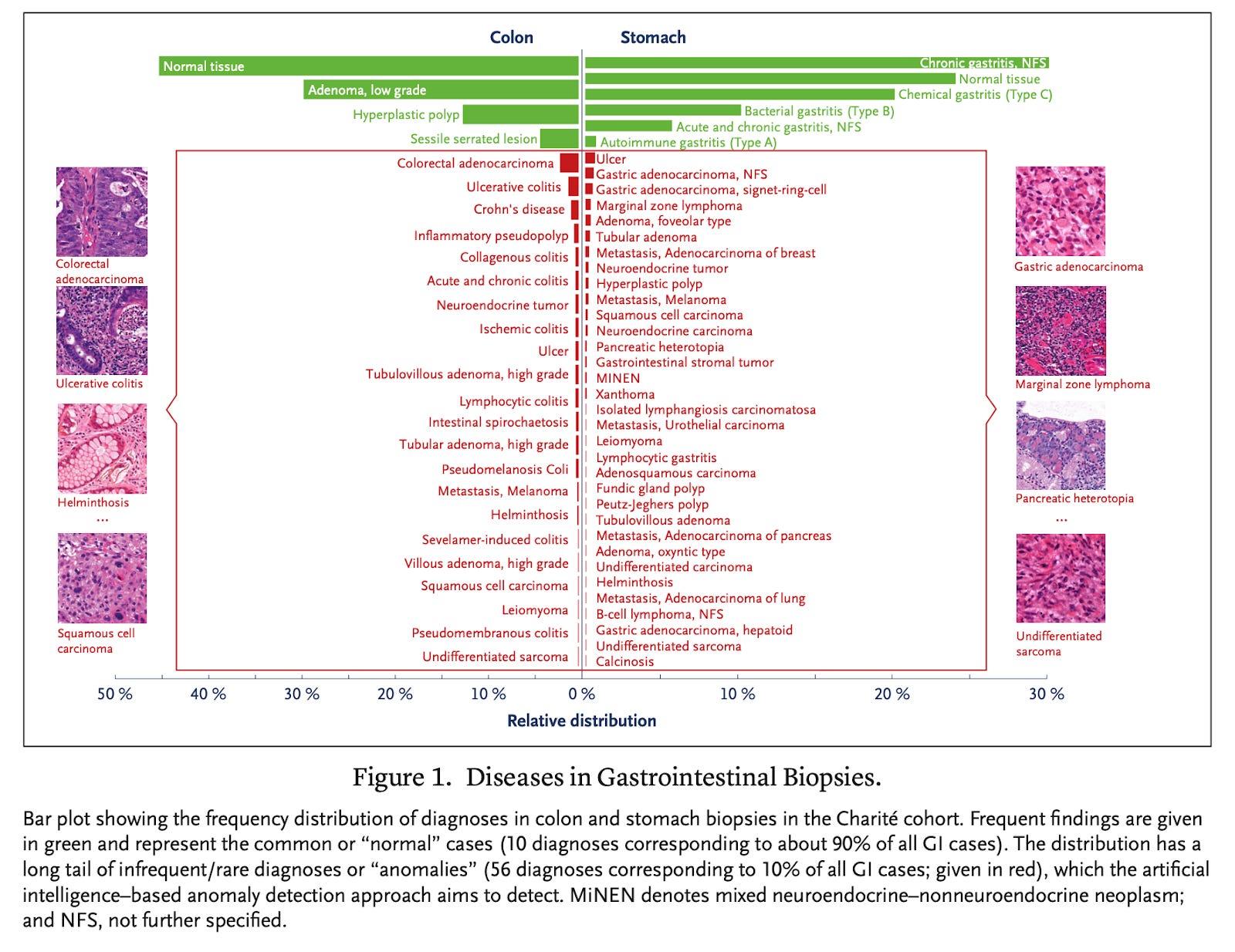
This is a huge issue when it comes to getting AI to recognize rare diseases. The paradox here is that “only a few diagnoses are common, and the vast majority of diseases are relatively rare,” as a recent NEJM paper notes. For that reason, AI training sets can’t possibly include enough examples of every rare disease that exists.
The paper reports on a way to solve the problem. Researchers focused on analysis of tissue samples from the gastrointestinal (GI) tract and used a method called anomaly detection (AD). Instead of trying to teach their model what every single GI disease looks like, they trained it to get exceptionally good at recognizing two things:
What does normal tissue look like?
What do the most common diseases look like?
Anything that didn’t fit into one of those two categories was labeled an anomaly - and flagged for review by a (human) pathologist.
The tool worked pretty well, especially for malignancies, where the best-performing model achieved 98% accuracy for stomach and 97% for colon.
COMMENTARY: This is an interesting and elegant way of avoiding the pitfalls of teaching an AI with an incomplete training set. Instead of ginning up artificial data to fill the gaps - a common technique that has its own set of problems - this team focused on leaning into what AI is really good at: synthesizing the huge amounts of data we do have. In this way, they created a tool that does what clinicians really want AI to do: Take care of the boring stuff so that they can focus on what’s interesting and clinically important.
Early diagnosis of early-onset cancers: How to get there?
Both serious (e.g., Nature) and tabloid articles (e.g., New York Post, UK Telegraph) have been describing what they call as an “epidemic” of early-onset cancers: Cancer that arises in folks under 50 years old. While these cases remain much, much rarer than cancers that show up later in life, any growth in these “prime of life” cases is a concern.
A Cell Reports Medicine review seeks to dig into what is causing this increase. Bottom line: We don’t really know what is going on (see all the variables in the graphic shown here). Given the lack of increase in heritable cancers, even the early-onset ones, the most likely suspect is the “exposome”: We are all exposed to far more cancer-permitting / cancer-enhancing drivers than people were in the past.
However, which elements of the exposome are more responsible for the growing cases and how exactly they drive onset are largely unknown. The dynamics are likely complex. A classic example here is a high-sugar / low-fiber diet, which can lead to obesity and diabetes - known cancer drivers.
What we do know, however, is that early-onset cancers have different molecular causes than later-onset cancers, and they progress faster. The differences in causality is critical, as it threatens the utility of personalized-medicine treatments, most of which were developed based on the molecular dynamics of late-onset cancers.
Separately, but very much related to early-onset cancers, the USPSTF (US Preventive Services Task Force) as well as ACOG (American College of Obstetrics and Gynecology) have issued new guidelines that recommend women begin mammograms at age 40, 10 years earlier than the current guidelines. The recommendation is now consistent with breast-cancer guidelines from other associations.

COMMENTARY: So can we diagnose these worrisome cases early enough to make a difference? Not well. Multi-cancer early detection (MCED) liquid biopsy has been touted as one solution to this problem, but as yet it’s inadequate. These tests have very low sensitivity for the earliest cancer stages (e.g., Galleri’s 8 - 23% sensitivity for Stage I solid tumors). When used to screen for a low-prevalence disease like early-onset cancer, a test with such a low sensitivity (i.e., lots of false negatives) will also deliver an overwhelming number of false positives. Results, in other words, will be meaningless.